
Complex Trauma and Pelvic Acetabular Injuries
Burden of disease:
Road traffic accidents are the leading cause of deaths worldwide. Globally, in 2019, there were 178 million new fractures (an increase of 33·4% since 1990), 455 million prevalent cases of acute or long-term symptoms of a fracture (an increase of 70·1% since 1990), and 25·8 million YLDs (years lived with disabilities) (an increase of 65·3% since 1990). The age-standardized rates of fractures in 2019 were 2296·2 incident cases per 100 000 population, and 5614·3 prevalent cases per 100 000 population. Complex trauma contributes significantly to the number of YLDs (years lived with disability) after road traffic accidents. It encompasses a wide spectrum of challenging injuries including but not restricted to high velocity Road traffic accidents, Gunshot injuries, Fall from heights and railway accidents.
Polytrauma (multi trauma) is a short verbal equivalent used for severely injured patients usually with associated injury (i.e. two or more severe injuries in at least two areas of the body), less often with a multiple injury (i.e. two or more severe injuries in one body area). Patients with multiple injuries are graded using a scoring system known as the Injury severity Score. The internationally accepted definition of Polytrauma is an ISS ≥ 16. It carries a mortality risk of above 10%. Some authors have suggested that at least two anatomical regions must be injured for a patient to be identified as having polytrauma. The ‘polytrauma’ definition using the Abbreviated Injury Scale (AIS) ≥ 3 for at least two different body regions seems more reasonable and feasible for identifying polytrauma patients. An international consensus meeting in 2012 first tried to define polytrauma by combining the concept of injuries in different body regions and parameters of physiological response. This new “Berlin definition” defines Polytrauma as ISS ≥ 16 and AIS ≥ 3 for at least two body regions along with at least one of the five standardized physiological responses (hypotension [SBP ≤ 90 mmHg], unconsciousness [GCS score ≤ 8], acidosis [base excess ≤ −6.0], coagulopathy [partial thromboplastin time ≥ 40 s or international normalized ratio ≥ 1.4], and age [≥70 years]).
Polytrauma management requires a well-developed and standardized management system or protocol, known as the Advanced Trauma Life Support (ATLS). This is a universal management system that includes combined evaluation and management of injured patients. The ATLS protocol consists of a primary survey, adjunct measures, secondary survey, and tertiary survey. The primary survey follows the ABCDE system that includes assessment and management of Airway, Breathing, Circulation, Disability, and Exposure.
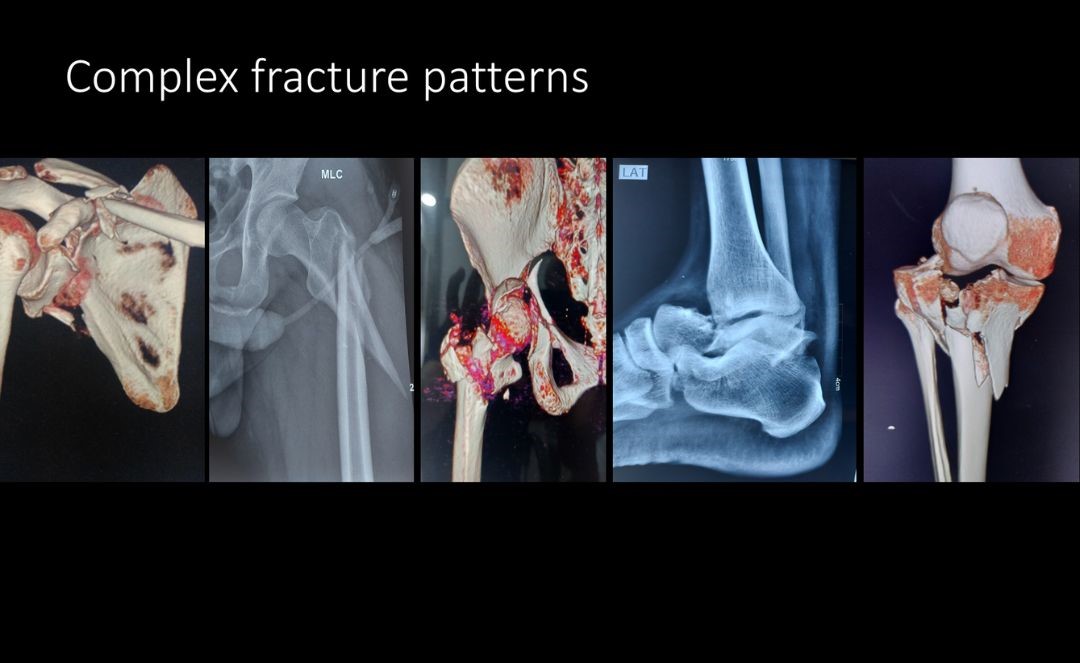
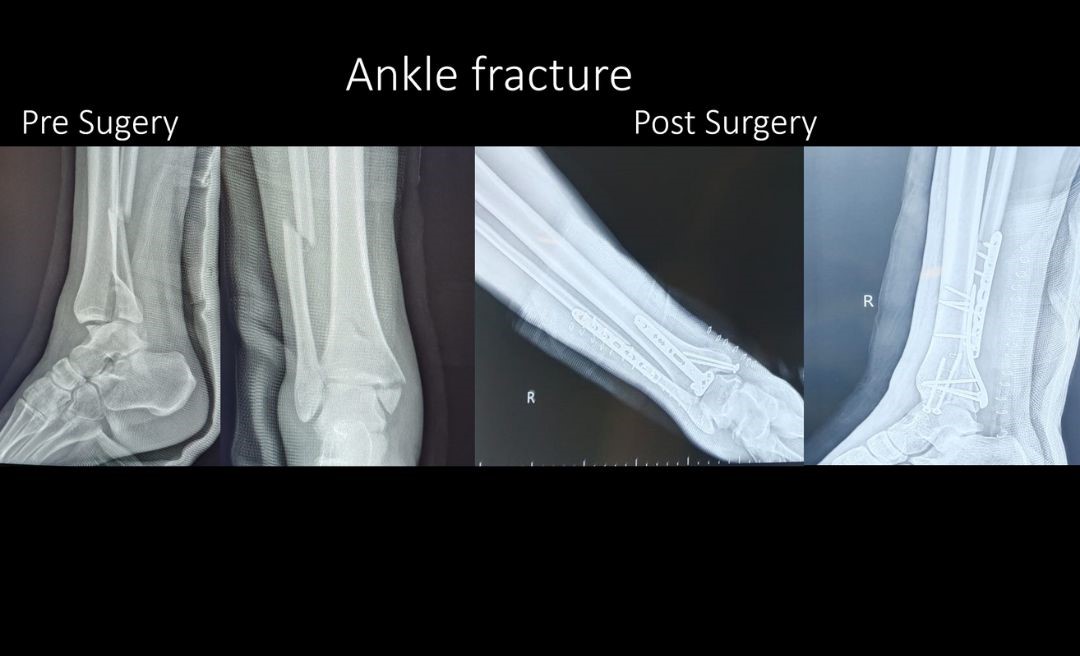
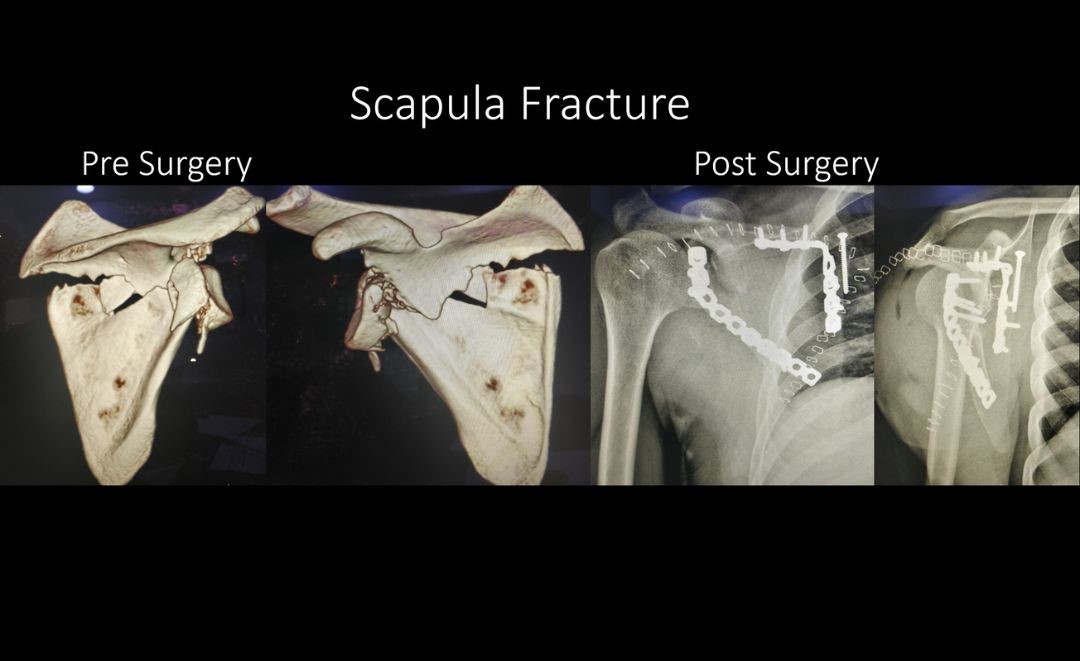
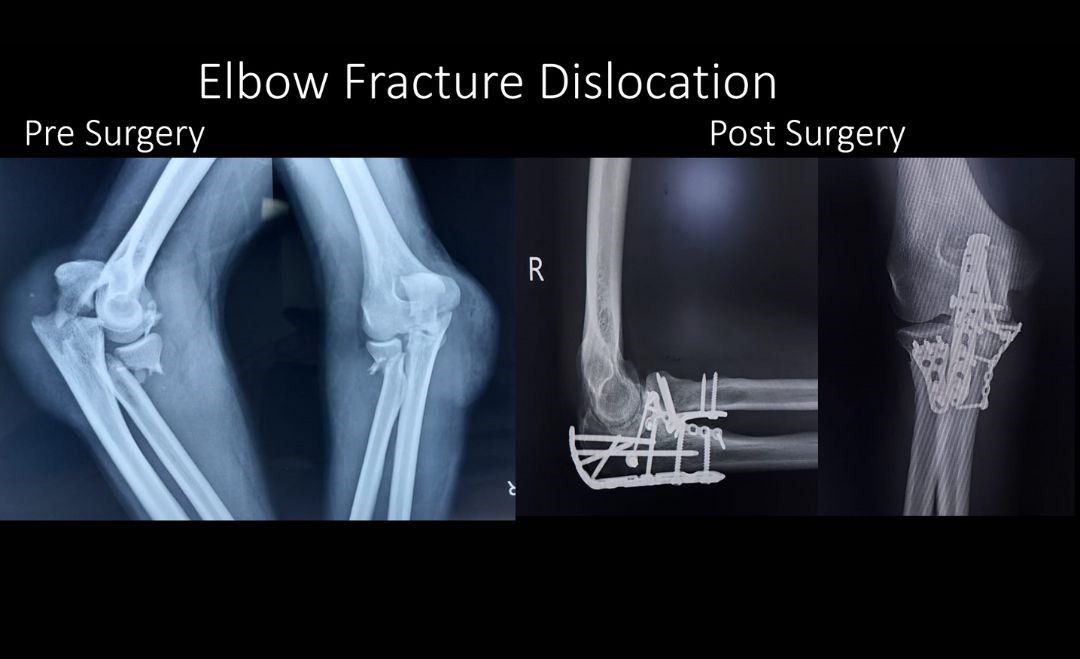
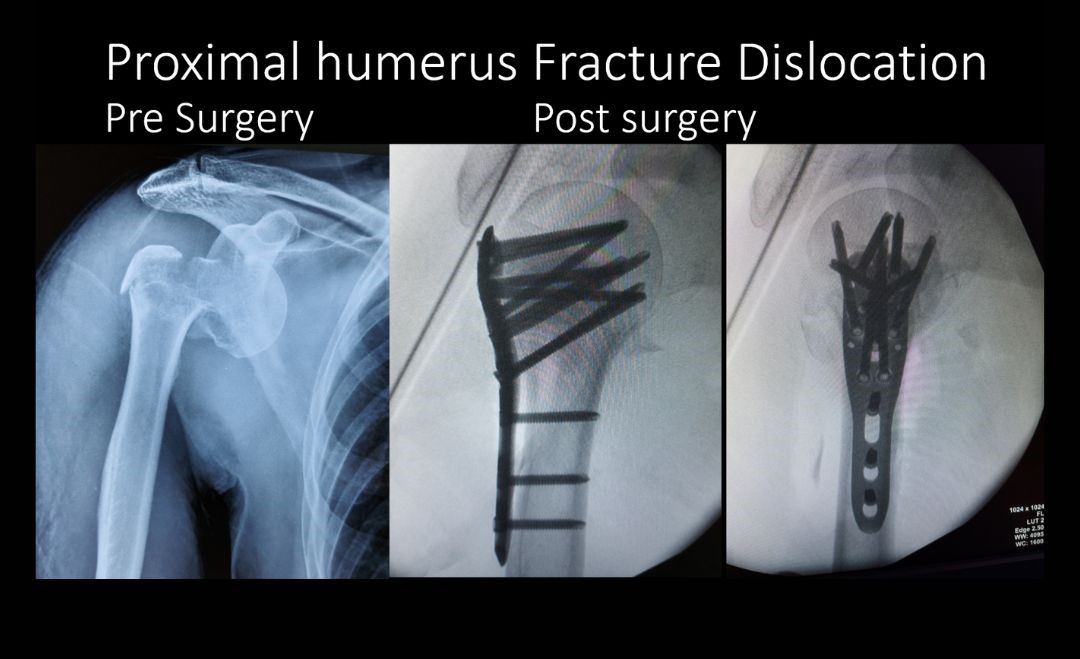
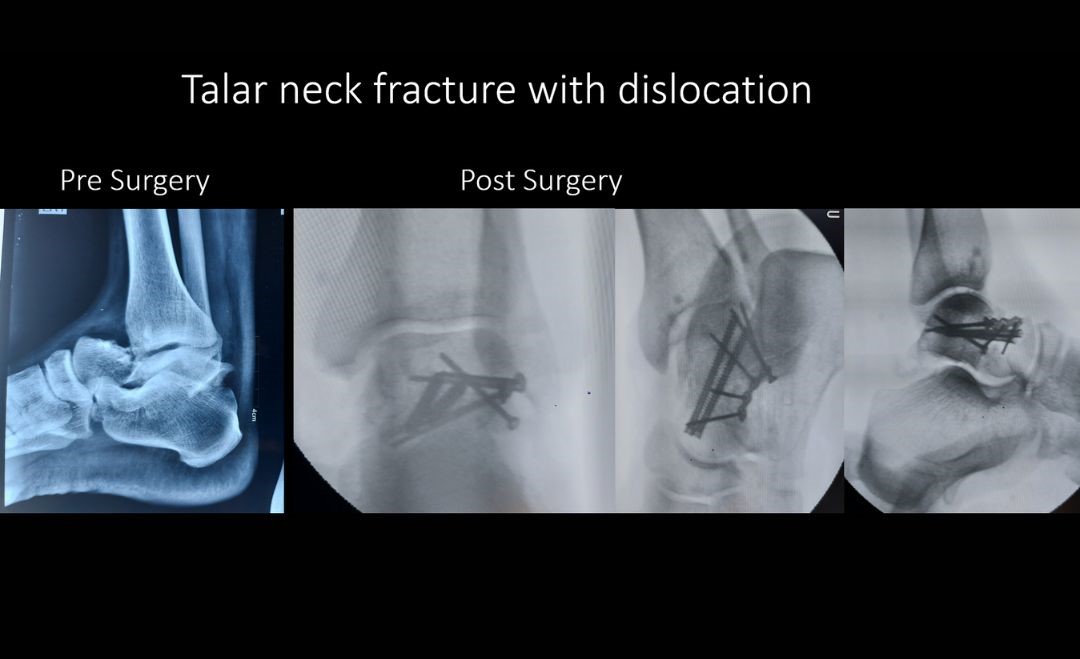
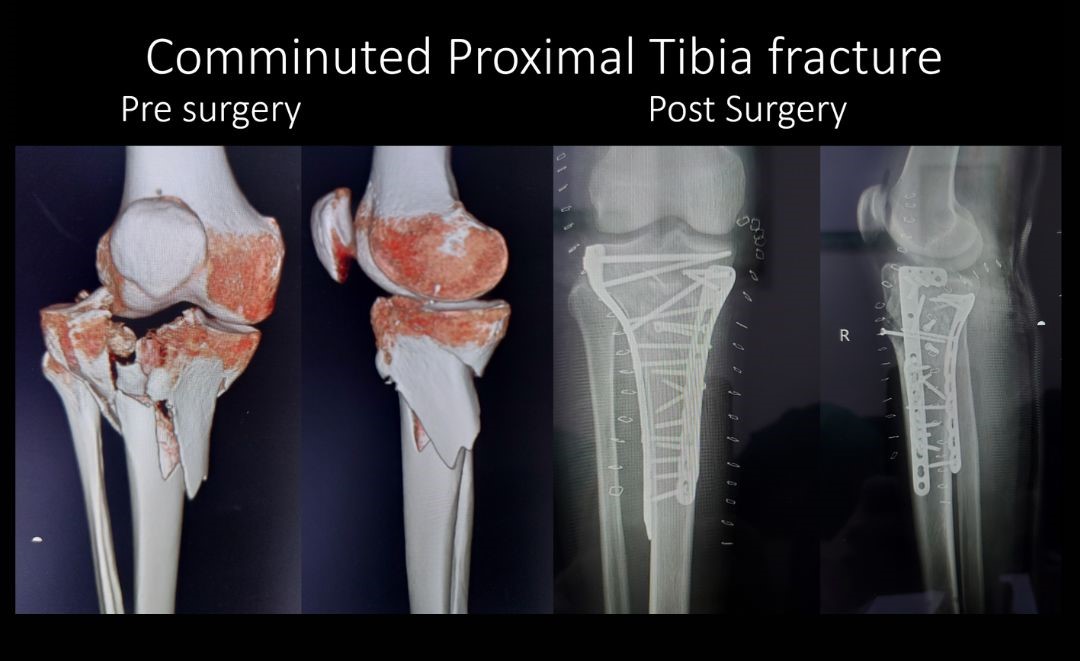
Complex Peri-Articular fractures
Periarticular fractures are the ones which either extend into the joint or are just adjacent to it. Accurate reduction and good fixation of such fractures is crucial for the joint to regain its function. Inaccurate reduction of the fracture is tolerated poorly by the joint leading to early arthritis. Assessment of soft tissue envelope surrounding the fracture is crucial. In the presence of extreme swelling and blisters, surgery should be deferred. Reconstruction of the joint surface many times requires multiple incisions simultaneously, and a healthy/ amenable soft tissue bed is a sine non quo. These fractures are associated with a relatively higher complication rate: wound infection, post traumatic arthritis, Joint stiffness, and risk of malunion. There is a high incidence of associated soft tissue and ligamentous injury in periarticular fractures around the knee. These injuries are usually addressed at a later stage.
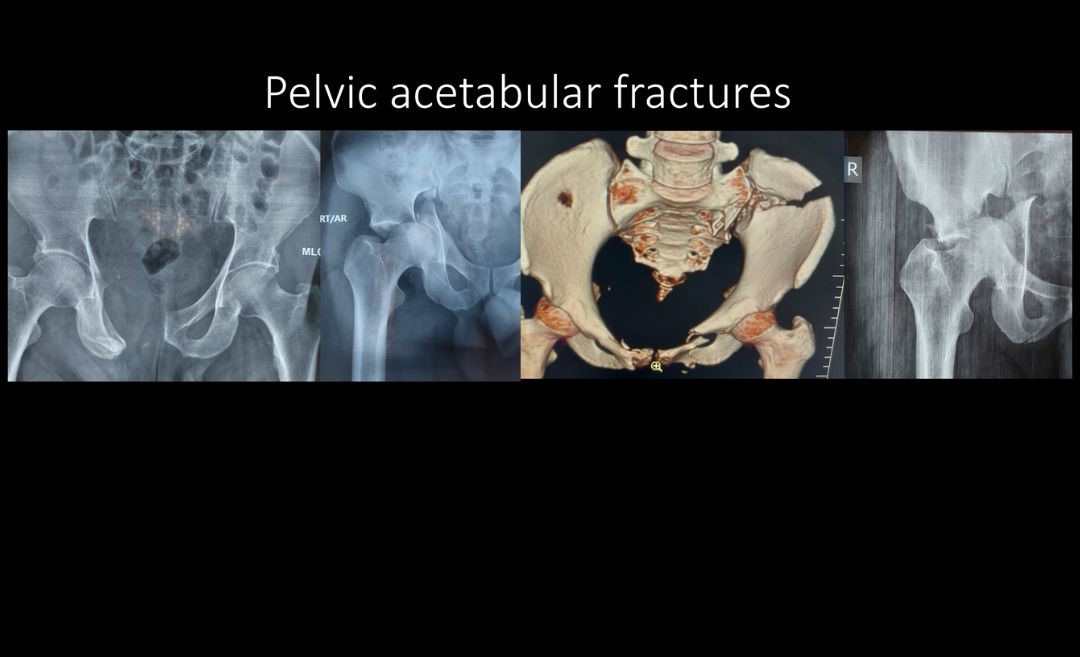
Pelvic acetabular injuries
The pelvis is made up of several bones (ileum, ischium and pubic bones) which create a bony ring. This ring serves as a connection between the spine and the legs. The ring is held in place and augmented at many places by important ligaments. It supports the weight of upper body and contains (and protects) many important vital structures like Urinary bladder, parts of large intestine, important blood vessels and reproductive organs. The acetabulum is the part of pelvic bone which articulated with thigh bone (femur head). The hip joint is a ball socket joint. The socket or the cup part is known as Acetabulum.
The majority of pelvic- acetabular fractures are caused by some type of high-energy event, such as a road traffic accident. Many of these patients have additional injuries that require immediate treatment. They are among the most serious injuries treated by orthopedic surgeons. Some elderly patients with fragile bones due to osteoporosis may sustain a pelvic acetabular fracture with a lower impact fall.
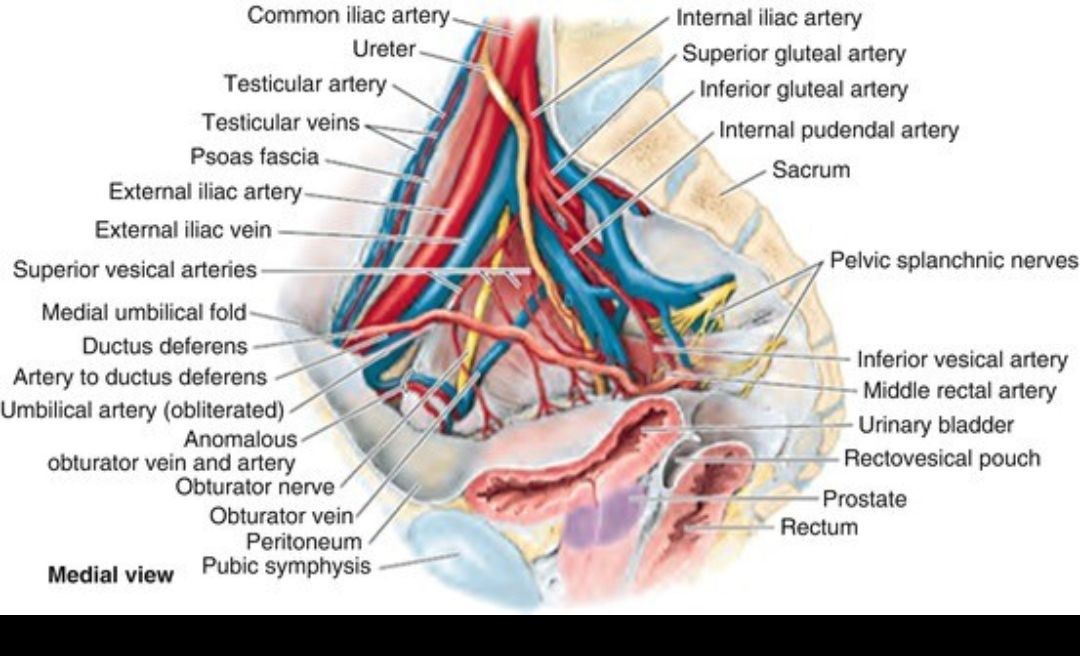
Fractures of the acetabulum are harder to treat because access to this bone is more difficult, and because of the acetabulum's proximity to the major blood vessels to the legs, the sciatic nerve, the intestines, the ureter and the bladder. Unlike a hip fracture, which can be treated relatively easily, to repair an acetabular fracture, the orthopedic surgeon, must, in essence, fix the broken bones from the inside out.
Patients with fractures of the pelvis and/or acetabulum, almost always also experience serious injury to surrounding soft tissue (skin and muscles- known as Morel Lavallee Lesion) and neurovascular structures (nerves, arteries and veins). In addition, especially in the case of pelvic fractures, adjacent organs can be seriously injured. With both types of fracture, there is significant bleeding and risk of nerve damage.
Treatment
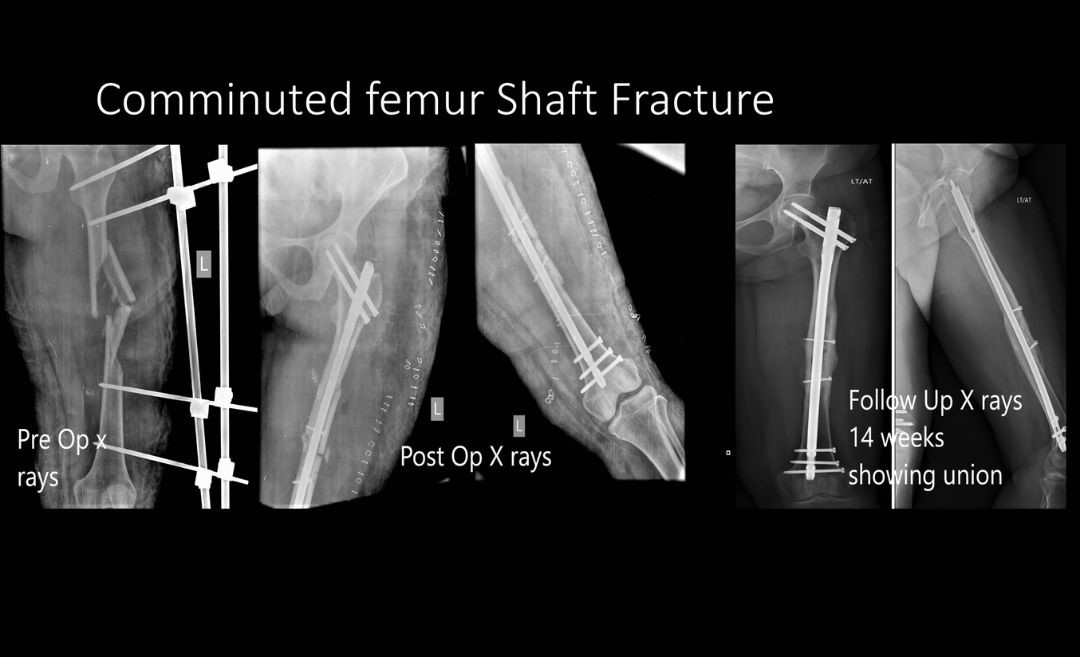
In patients with multiple injuries and accurate and rapid initial assessment of injuries is done in the Emergency room and treatment is started simultaneously. The priority sequence is based on the ATLS protocol and includes securing Airway, Breathing, Circulation and Disability management. A multidisciplinary approach is the key and includes- Trauma Surgeons, General Surgeons, Orthopedic Surgeons, Neurosurgeons, Intensivist Anesthetist and Nurses. During the early phase the aim is to stabilize the general condition of the patient so that a detailed and accurate assessment of injuries can be done at a later stage (Secondary survey). During this early-stage Damage control surgeries may be performed which include placement of Temporary External fixators on the leg and/or pelvis. These are often lifesaving surgeries which are performed quickly with the aim of stabilizing a deteriorating patient.
Once the patient is stabilized – bleeding has stopped, and other life-threatening injuries have been addressed – the fractures can be treated definitively. Because of the complex nature of these fractures and because many orthopedic surgeons do not regularly treat them, patients who initially go to a community hospital for emergency attention are often transferred to an institution that specializes in such injuries.
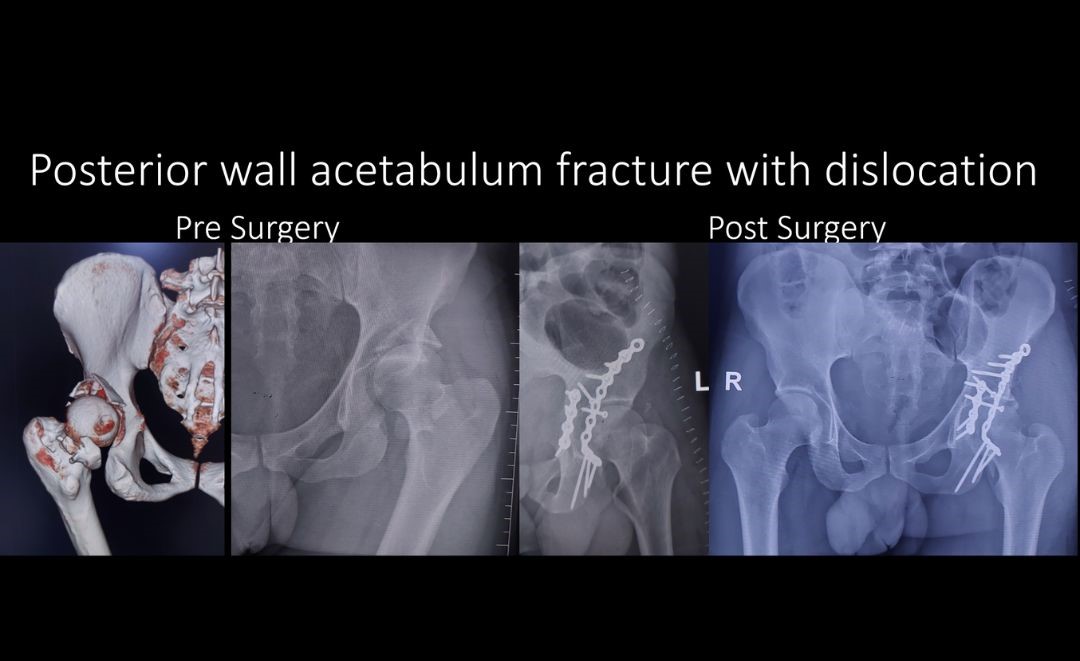
Accurate reduction of periarticular and acetabular fractures is of paramount importance. Inaccurate reduction can lead to progressive joint damage and premature post traumatic arthritis. Reduction of fracture fragments is usually done by opening the fracture site- hence the name Open reduction is often used by Orthopedic surgeons. Once the bones are realigned, the surgeon uses internal or external fixation to hold the bone in proper position during healing.Metallic devices including wires, Interlock Nails, screws, and plates are used.Patients are encouraged to get up and out of bed as soon as possible, since doing so helps to avoid some of the complications associated with these injuries. A regimen of physical therapy is followed to maintain muscle strength and range of motion during recovery.
