



Etiology/ causes
Pediatric
Deformed limbs may be due to congenital anomalies (by birth) or due to defective development of the bones during growing phase. Congenital anomalies are usually easily recognized. Some of the common congenital anomalies include Clubfoot (CTEV) and Dysplatic Hips. Deformities secondary to Cerebral palsy and Brachial plexus injuries may present a little later.
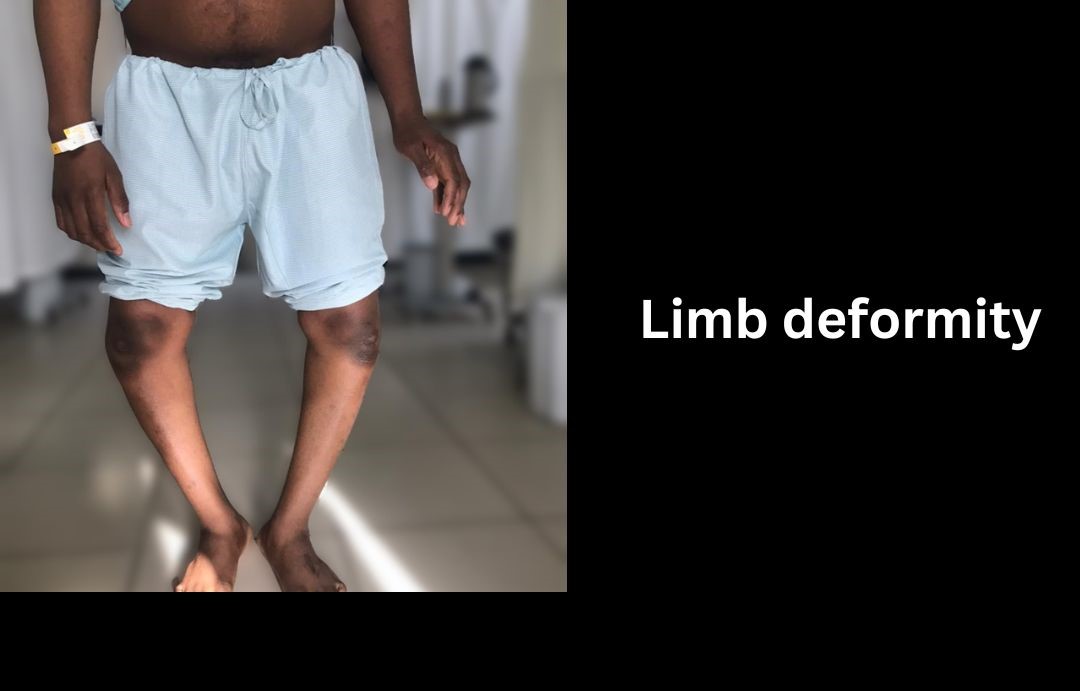
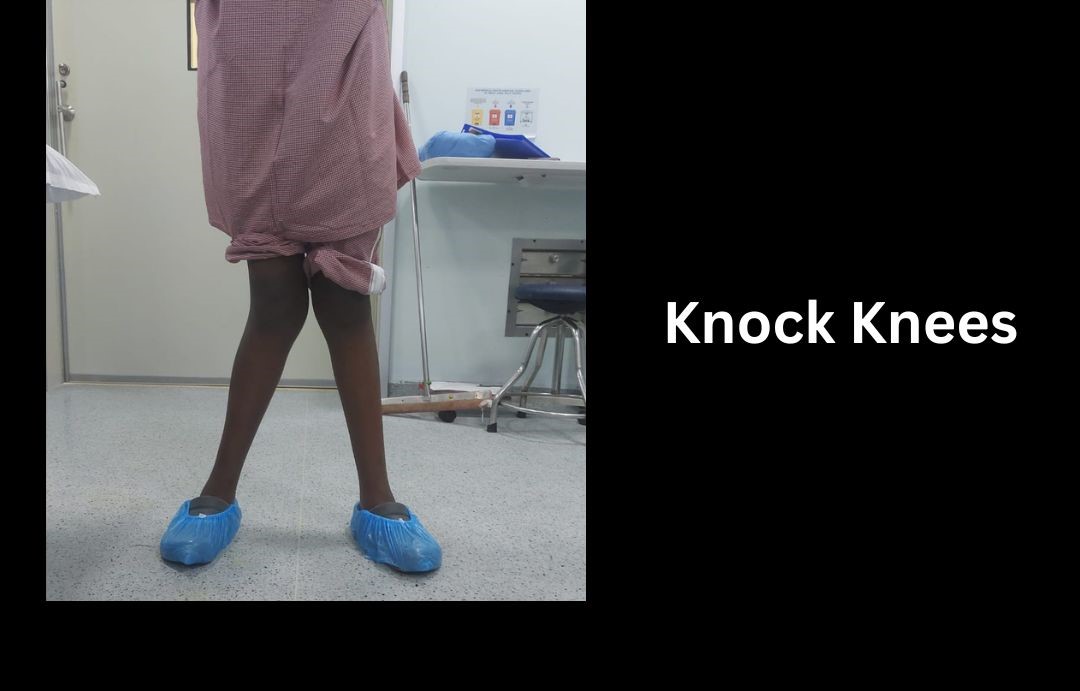
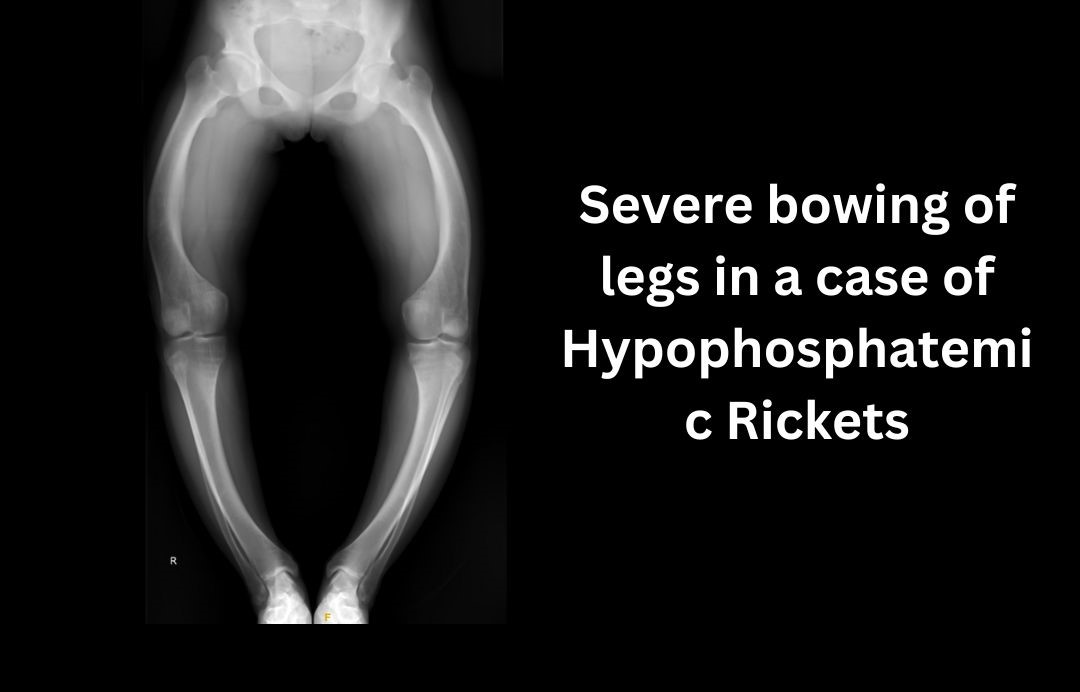
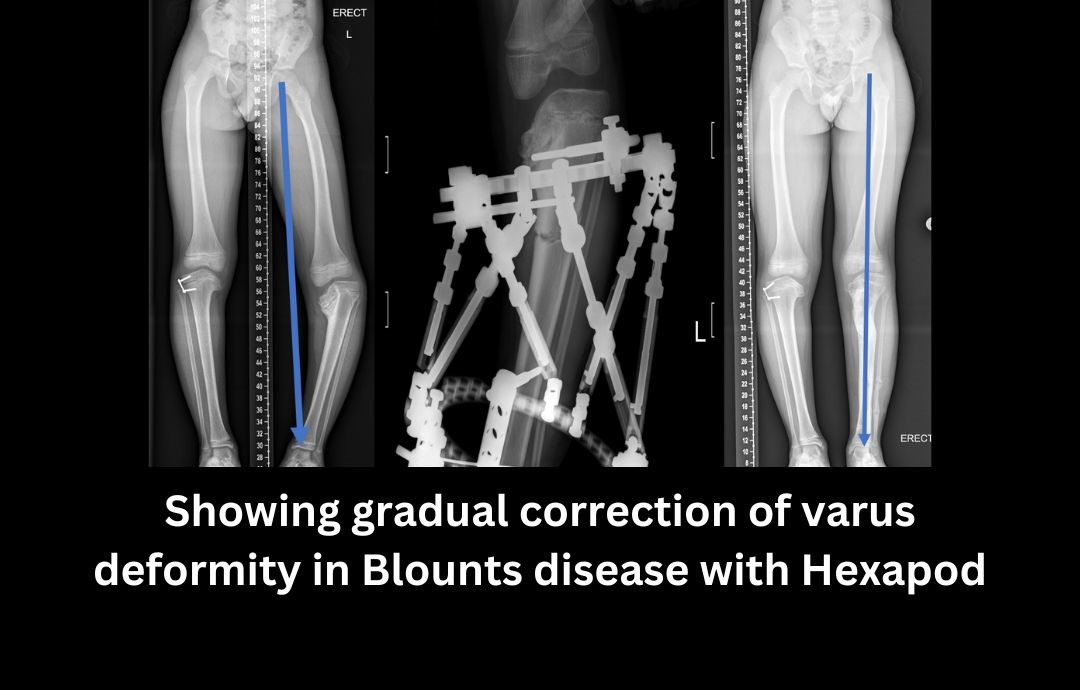
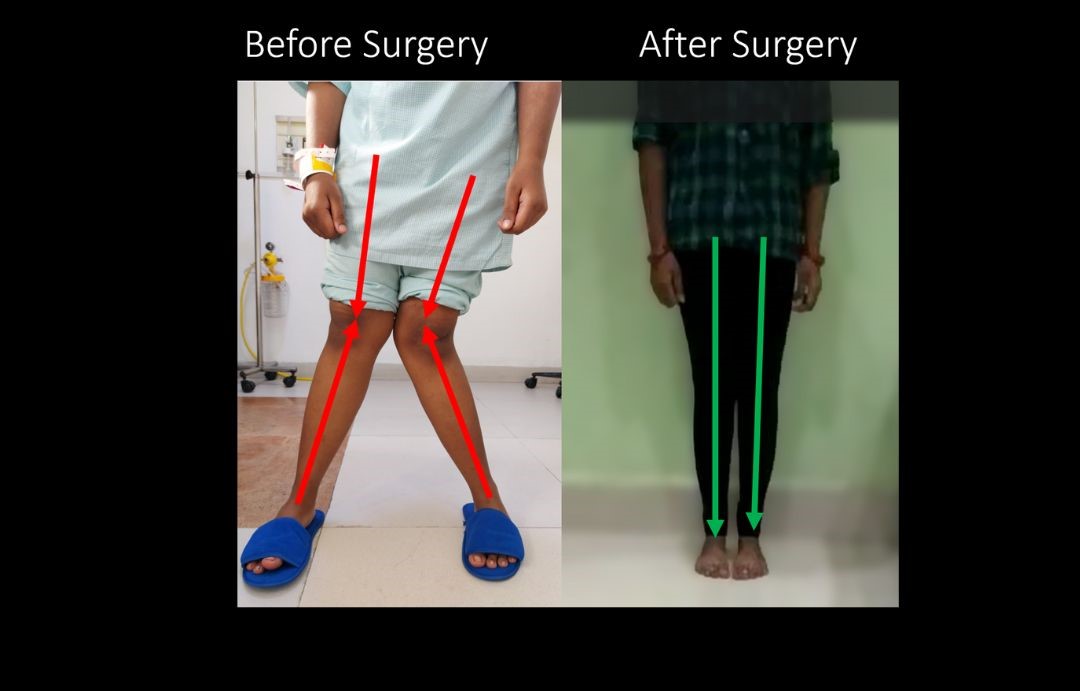
Knock knees and Bowlegs are one of the commonest deformities seen during adolescent or growing phase in children . They are usually secondary to low Vitamin D levels (Rickets) which in turn leads to growth abnormalities. Low Vit D may be secondary to dietary deficiency or metabolic disorders like Hypophosphatemic Rickets. Abnormal pressure on the growing physis (place of bone growth in children at the ends of long bones) due to obesity or malnourishment can also result in bony deformities in children. Trauma and fractures around Growth plate in children can lead to limb deformity which may increase as the child grows. They may become apparent years after the initial injury. Cubitus Varus is a common deformity of the elbow seen in children after malunited distal humerus Supracondylar fracture. They present with classic Gunstock deformity of the arm. Blount’s disease is a condition that affects the proximal Tibia growth plate. Its common in children of Afro-Asian descent . The disease causes the growth plate near the inside of the knee to either slow down or stop making new bone. Meanwhile, the growth plate near the outside of the knee continues to grow normally. The result is a bowlegged appearance in one or both legs. Blounts disease may present in the first 2 years of birth (Infantile Blounts) or around 10 years of age (Adolescent Blounts). Children with infantile Blount’s disease are typically early walkers (prior to 12 months) and are often overweight. Adolescent Blount’s disease may be related to rapid weight gain or obesity. There is also believed to be a genetic component in development of Blounts disease.
Adults
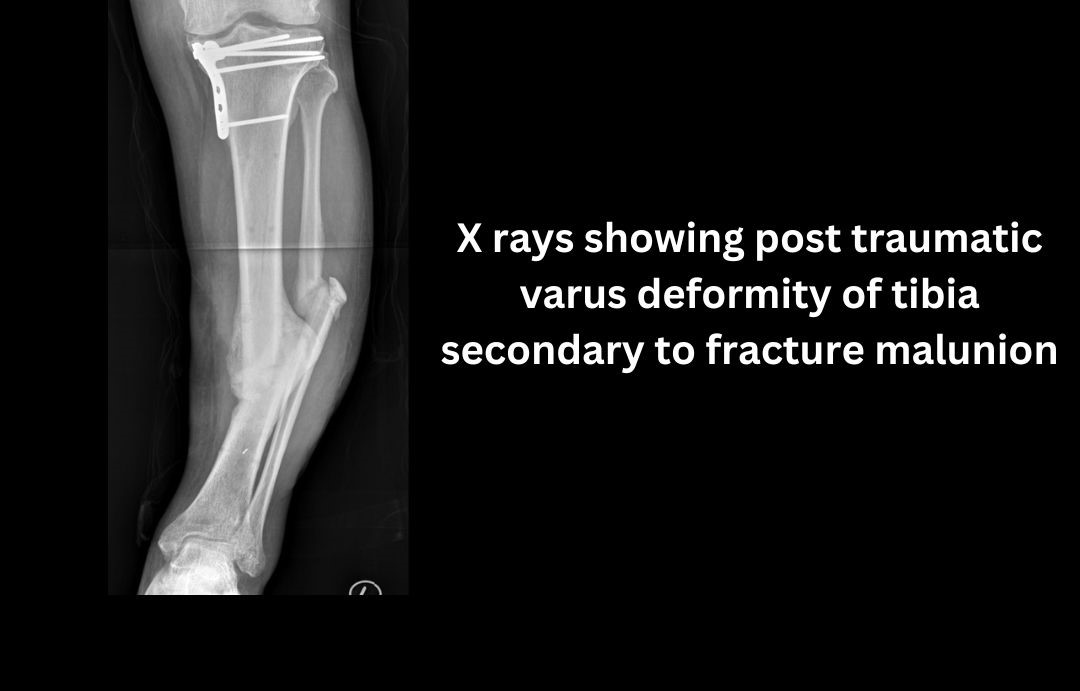
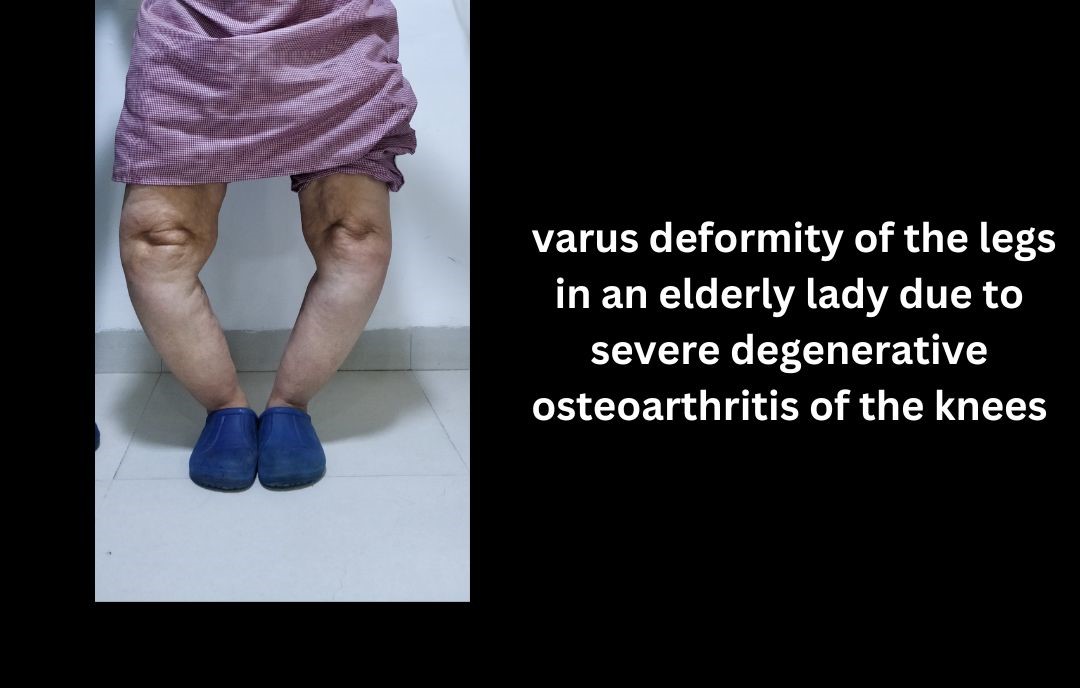
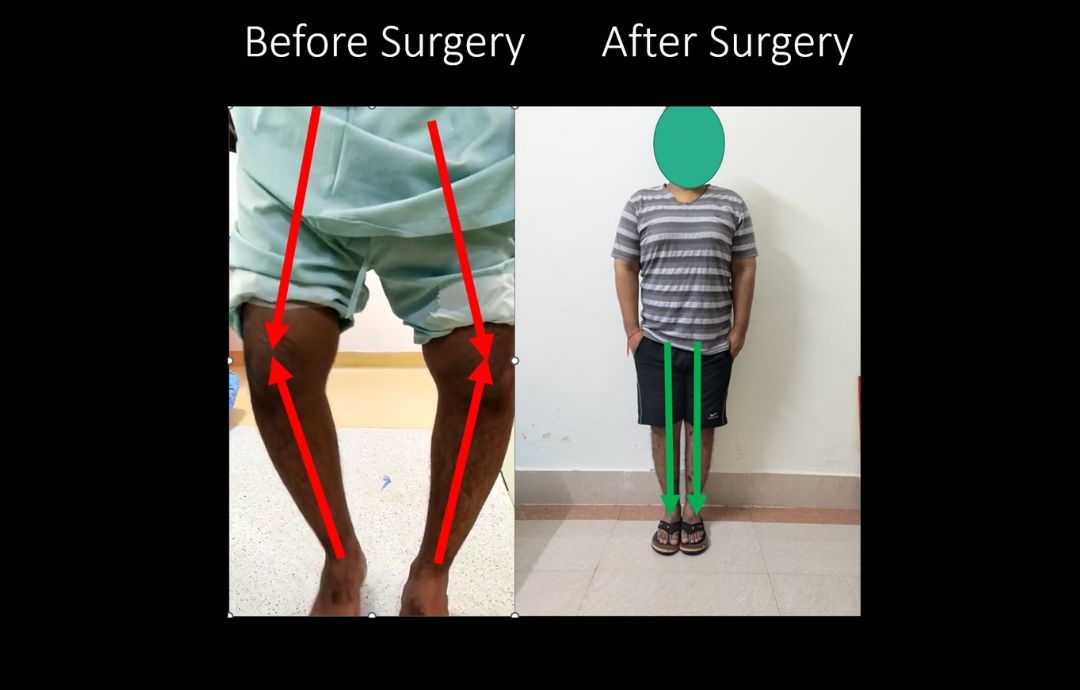
Trauma or malunited fractures is the leading cause of deformity in adults. Other causes of adult deformities include neurogenic disorders like peripheral nerve injuries, Stroke, Charcot Marie Tooth disease, Poliomyelitis etc. Bowlegs in adults is usually due to degenerative arthritis of the knee joint .
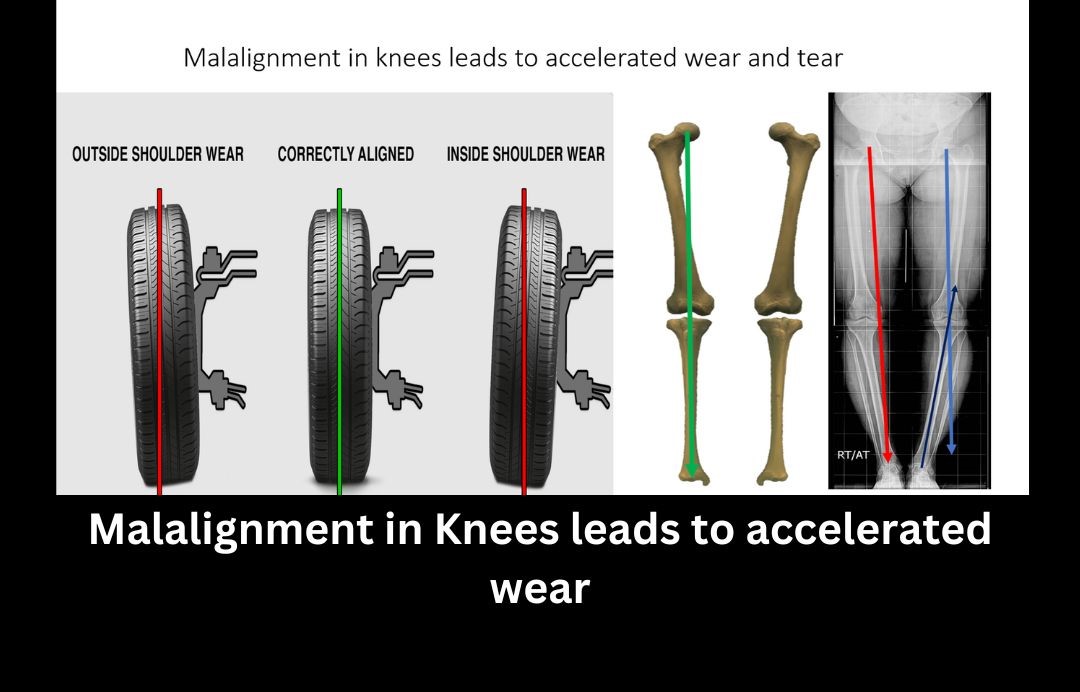
Regardless of the cause of deformity- it can severely impair functioning of the limb apart from being cosmetically appalling. Deformity of the legs in the long term can lead to arthritis of the joints as there is uneven distribution of the body weight on the joints. It’s akin to accelerated wear of a car’s tyre due to malalignment.
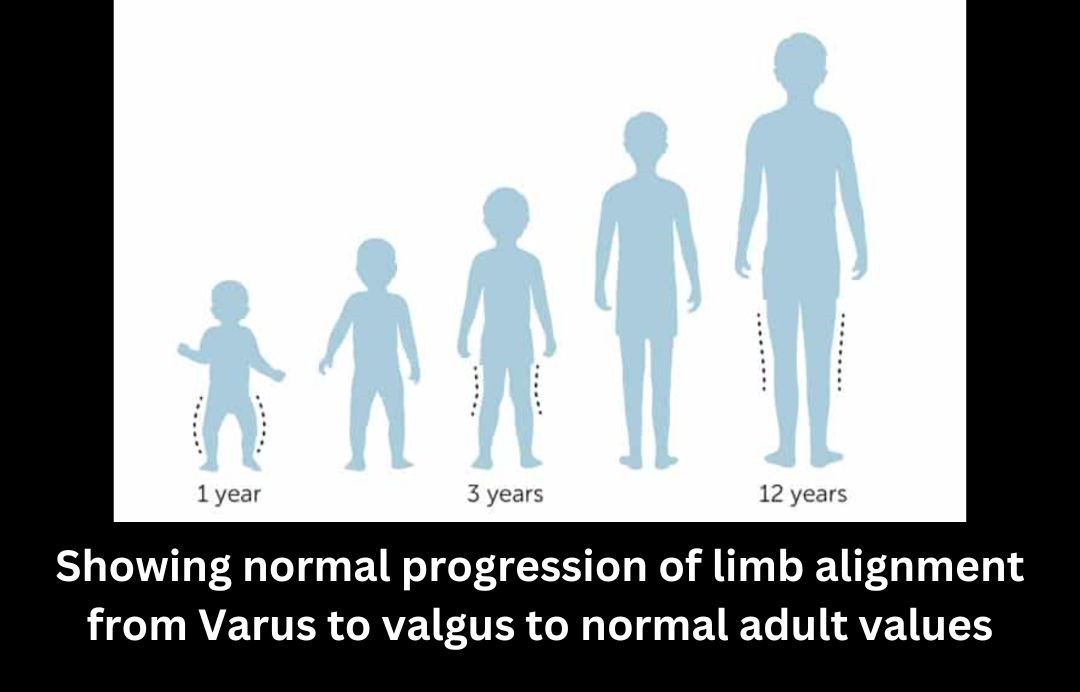
Normal Alignment- progression of normal alignment with age
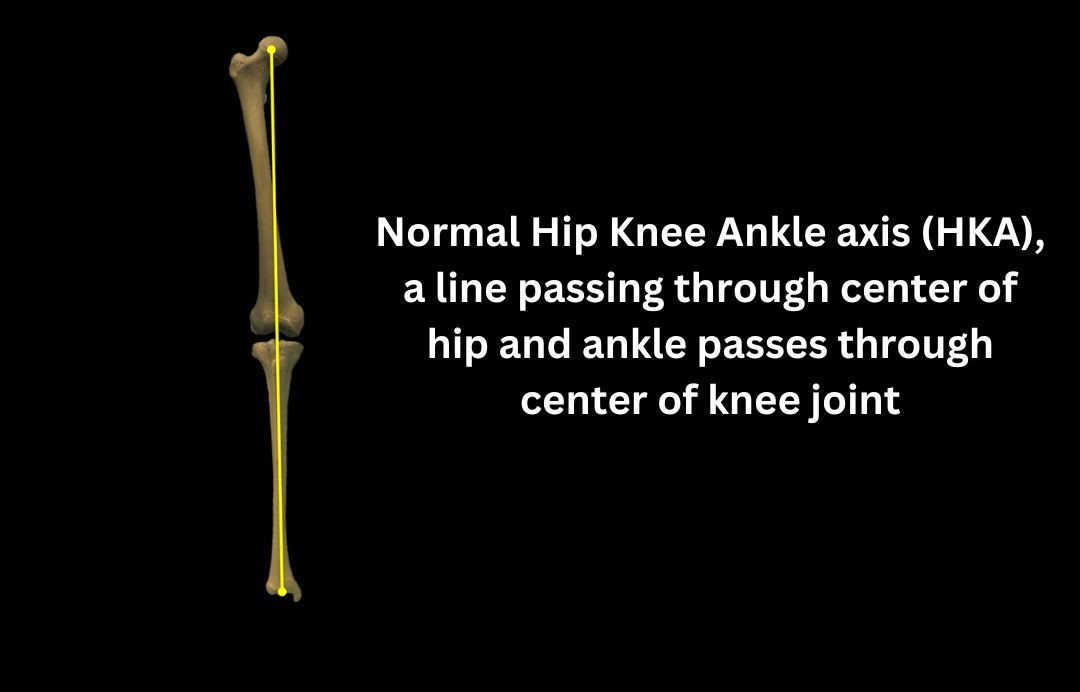
As children grow from toddlers to teenagers, normal alignment changes occur in their legs . Most children are naturally bowlegged when they start to walk. Usually by the age of 2-3 years, the legs start to look more like knock knees. The knock knee phase peaks in the next 1-2 years. After six years of age the knees will normally assume a straighter alignment and there should be very little change in the angular growth. By 12 they have grown into what will be their adult configuration. In adults, the Hip center, knee center and ankle center lie in almost straight line. The HKA axis (Hip, Knee, Ankle) as it’s commonly known has a variation of around +/-3 degrees . Alignment falling outside this zone needs to be addressed often.
Treatment
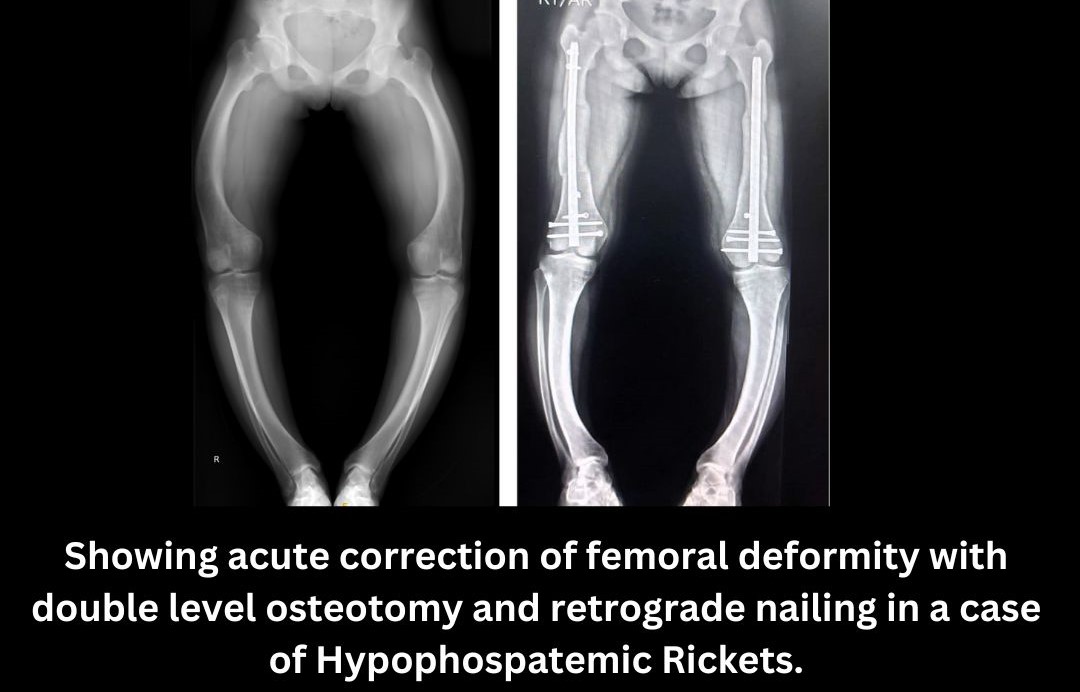
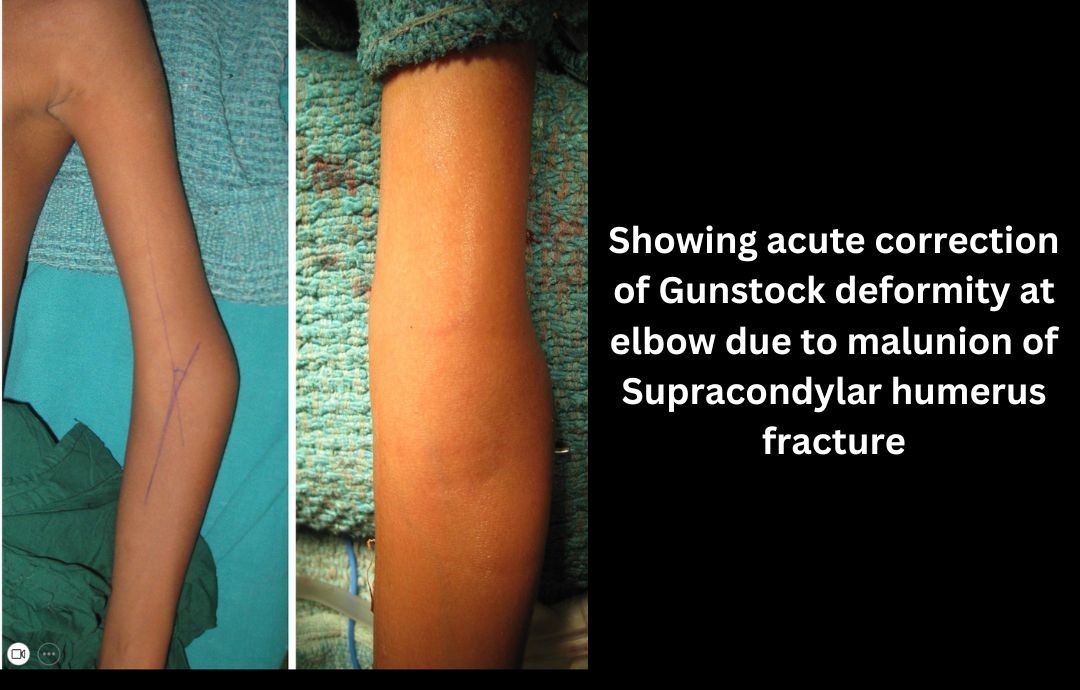
Identifying the underlying cause of deformity is important, especially in metabolic disorders. Correcting the underlying Vit D deficiency or metabolic profile is of paramount importance. Deformity correction may be done acutely or gradually. Acute correction involves bone osteotomy and fixation with either a plate or intra-medullary nail. Small deformities are amenable to acute corrections. Femoral deformities are especially suitable for acute corrections as risk of nonunion is less and tolerance of femoral external fixators is relatively poor. Acute correction of Gunstock deformity of arm or Cubitus varus after malunited supracondylar fractures also gives excellent results .
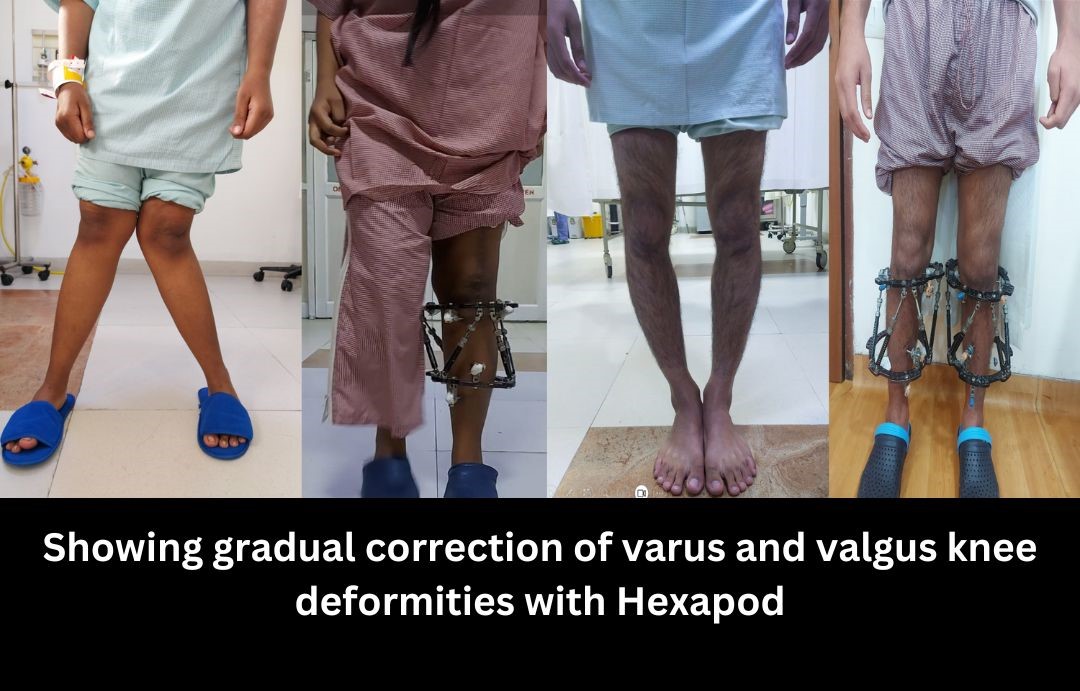
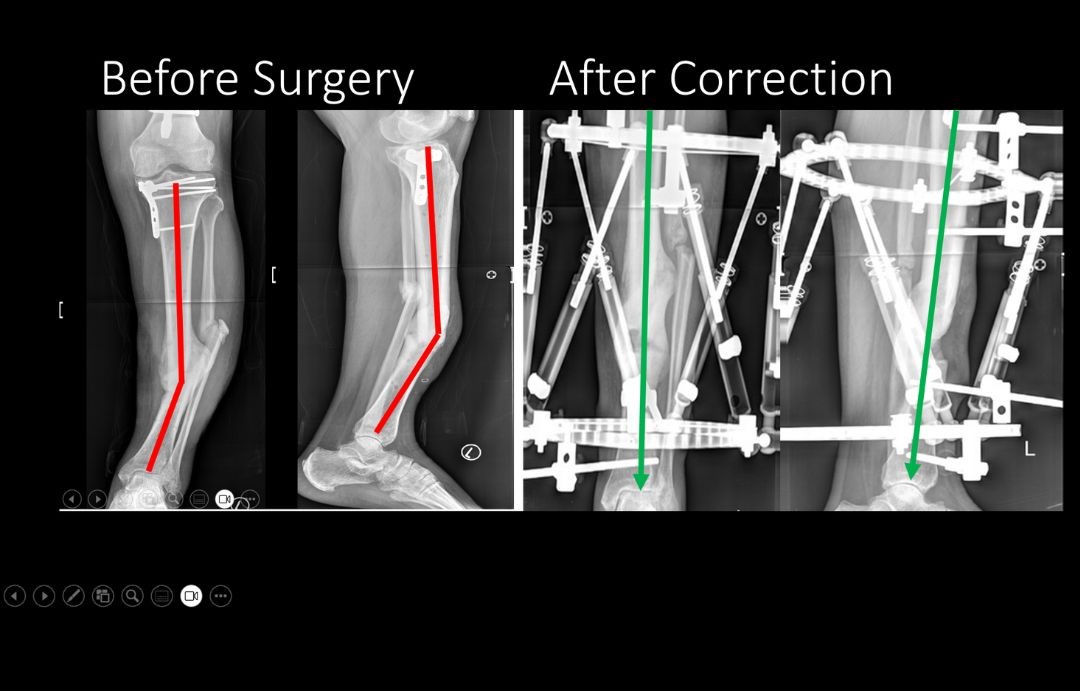
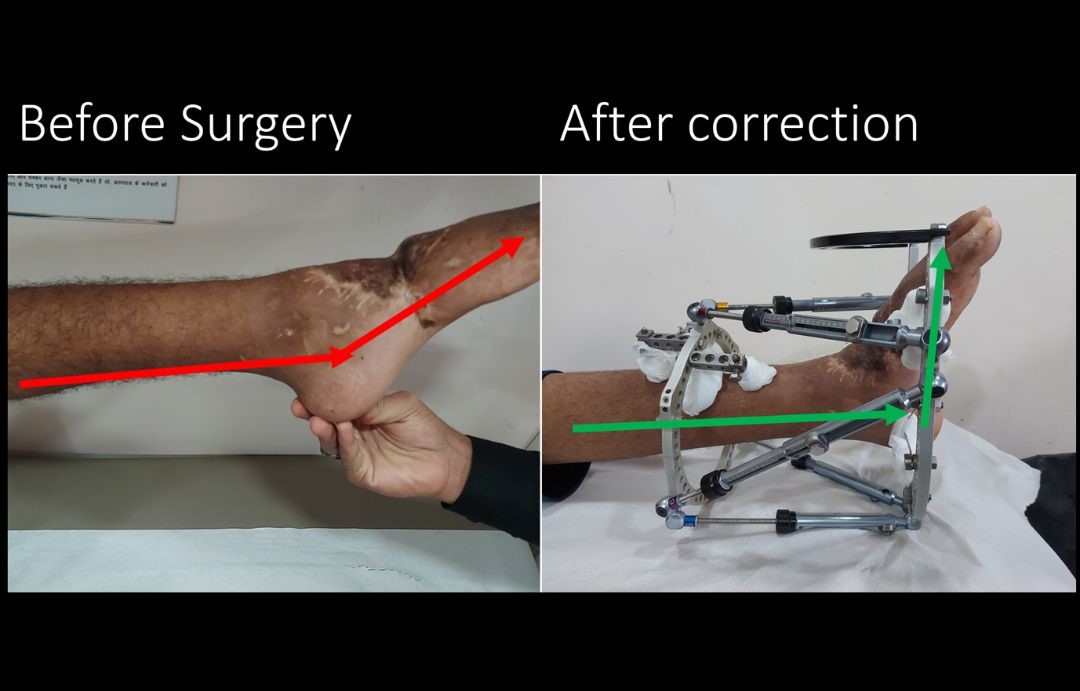
Gradual correction involves osteotomy and application of an external frame/ Fixator. Gradual correction is needed when deformity is large. It’s also done when lengthening of the limb is required. Acute correction may seem more convenient. However, gradual correction with frames is more accurate since it allows the surgeon to correct the deformity in post op period till perfect correction is achieved.
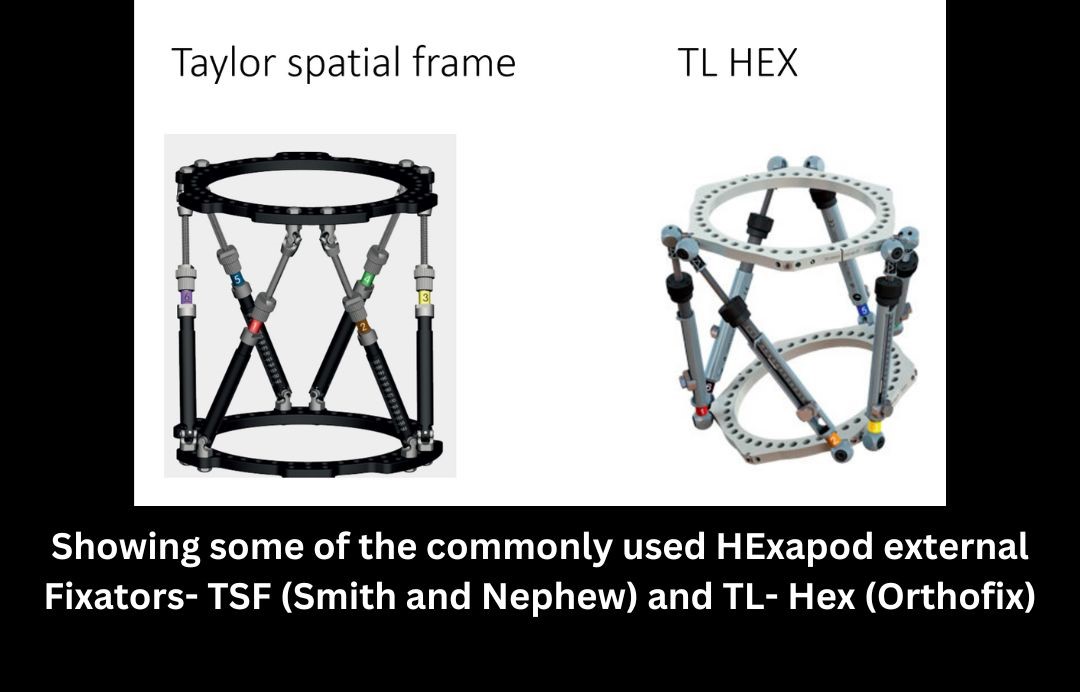
Gradual deformity correction usually involves application of circular external fixators with 6 connecting struts between the rings. Hence the name Hexapod. The first clinical usage of hexapod fixators in medicine was in 1995, when J.C. Taylor introduced his “Taylor Spatial Frame,” to perform complex limb deformity correction. Many hexapod fixators have been since introduced. Hexapods are powerful tools which allow simultaneous correction of deformity in all three planes as well as lengthening of the limb. All Hexapods use the conventional Ilizarov principles for fixation to bone. However, they are much more convenient to use, both for the surgeon as well as the patient. The Hexapod struts can be adjusted with hand as compared to the need of spanners for conventional Ilizarov apparatus. Hexapods allow simultaneous correction of deformity in all three planes which obviates the need for frequent changes in hinge placement and frame configurations which is required in conventional Ilizarov apparatus Despite many differences, all the principles of frame stability and fixation construct of Ilizarov apparatus are applied to Hexapod devices.
Minimally invasive deformity correction
Gradual correction of deformity in children who have enough growth potential left can be done in a minimally invasive method. It involves the application of an eight plate on one side of the growth plate to modulate the child’s growth. The procedure is extremely simple, safe and easy way to correct bow legs and know knees in relatively younger children. It’s done on a day care basis and the child can perform all activities of daily living almost immediately. A close follow up is necessary and the eight plates are removed once the deformity is corrected.
Role of 3D printing in deformity Correction
3D-printing is a promising adjunct in the armamentarium of orthopedic surgeons and is especially useful for deformity correction. Accurate bone models specific to patients’ anatomy can now be prepared using CT scans and 3 D printing machines. These bone models help the surgeon to understand the complex deformity better and allow simulation of the surgical plan on the bone model. Patient specific bone cutting jigs can also be made, which help the surgeon to make accurate bone cuts. 3 D printing is especially useful in understanding and planning correction of complex foot and ankle deformities .
